
More than one calculus in submandibular duct is a rare finding. Interestingly a case of multiple sialoliths in Wharton’s duct reported to the department which was managed by intraoral incision and retrieval of sialoliths thrice. Recurrence of multiple sialoliths in the duct was revealed in the long term follow-up, eventually leading to sialadenitis of the gland. Extraoral excision of the submandibular gland had to be performed in this case.
The management of sialoliths is decided based on the topography of the gland, the size and number of stones, the functional state of the gland, the degree of superinfection and the surgeon’s technical skill.
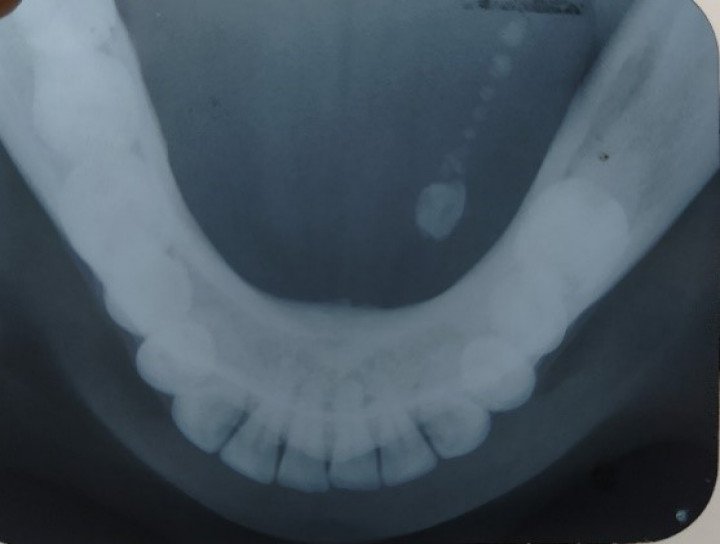
Sialolithiasis of submandibular gland can be managed by intraoral excision of ductal calculi with linear incision on the mucosa along the duct which makes the calculus bulge and then it is removed. While following this procedure, care must be taken not to exceed the first mandibular molar to avoid lingual nerve damage. In order to avoid its posterior migration during surgery a traction suture is placed behind the calculus which is very important for a successful surgery. This case was performed with this same intraoral technique thrice along with insertion of infant’s feeding tube to maintain the patency of the duct. However, multiple recurrences led to sialadenitis of the gland four years after first surgery. Decision was taken for extraoral excision of the submandibular gland. Submandibular approach was used for excision of submandibular gland along with the Wharton’s duct.
The wound healed uneventfully after successful excision of the gland.
No Any Replies to “SIALOLITHIASIS OF WHARTON’S DUCT”
Leave a Reply