
The long-term goal of implant therapy is to prevent or to arrest the progression of disease and to achieve a maintainable implant site.
Endosseous dental implants have revolutionized the field of periodontics. During the last decade, a great deal of information has been generated concerning the effectiveness and predictability of endosseous implants. Implant placement is a viable option in the treatment of partial and full edentulism and has become an integral facet of periodontal therapy. The long-term goal of implant therapy is to prevent or to arrest the progression of disease and to achieve a maintainable implant site.
With the increased use of osseointegrated implants and with many implants functioning for long periods of time, the soft tissue barrier around implants has become more important. Improvements in implant surface technologies, surgical instrumentation, and prosthetic connections and restorative materials have greatly reduced hardware associated complications.
Implant complications can be due to a number of causes including prosthesis instability, implant mobility, occlusal trauma, fractured components, pain, inflammation, infection, and neuropathy.
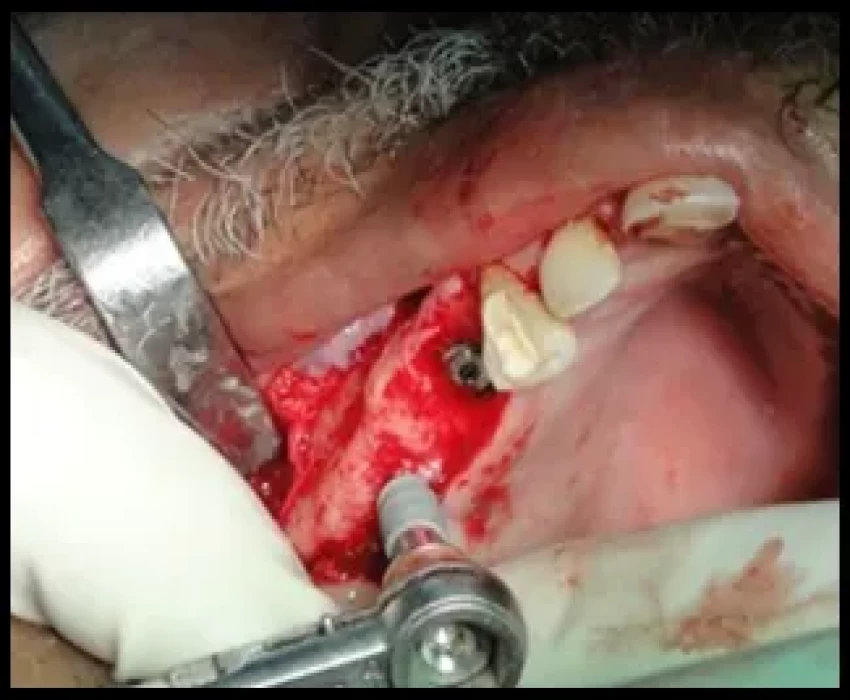
The intraoperative complications related with surgery, hemorrhagic accidents occur most frequently in the interforaminal region, since the majority of the vascular branches enter the mandibular bone in this region. Nerve damage can arise as a consequence of inferior alveolar nerve transposition or lateralization, or the excessive intrusion of drills or implant fixture into the mandibular canal. Mandibular fractures secondary to implant placement occur more easily when placing implants in atrophic mandible. Occasionally, incorrect positioning or lack of relative parallelism in the placing of the implants causes damage to an adjacent tooth. Absence of primary stability may occur as a result of overworking the implant bed during preparation, also to poor bone quality, and more frequently to immediate post-extraction implantation. Another possible complication is the migration of implants into the maxillary sinus.
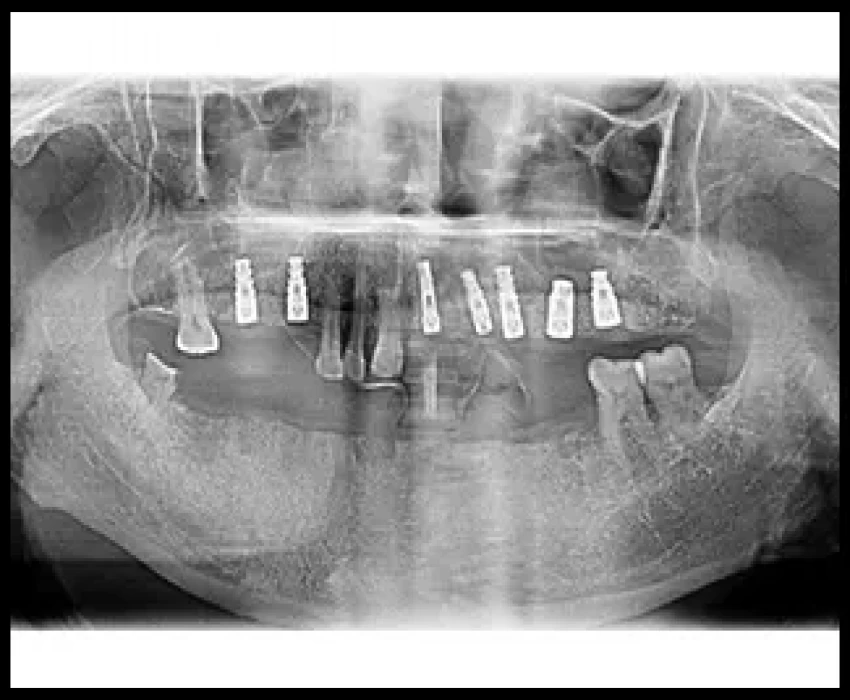
Peri-implantitis is considered as one of the important postoperative soft tissue complications associated with implant placement. Depending on the severity of the peri-implant bone loss, the morphology of the bone defect and the implant surface, the progression of the disease process can potentially be arrested and in selected cases, the lost bone tissue can be regenerated.
An attempt has been made to review various complications related to implant therapy, with a particular emphasis on peri-implant diseases, including its diagnosis and management.